For 16 of the last 23 years, the NDP has governed Manitoba in accordance with its progressive or left-of-centre ideology. Progressive parties are usually more supportive of gender ideology and medical gender transitioning than their conservative counterparts.
Is this apparent in Manitoba’s policies, providers, and prevalence of medical transitioning for minors?
Yes. Manitoba liberally provides medical gender transitioning for minors. Though governed the longest by progressive governments in this century, Manitoba’s approach to gender medicine is similar to that of other Canadian provinces, with the recent exception of Alberta.
Policy
One of the main purveyors of pediatric gender medicine in Manitoba is the Gender Diversity and Affirming Action for Youth (GDAAY) clinic next to the Winnipeg Children’s Hospital. The clinic has a multidisciplinary team that includes a pediatric endocrinologist, an adolescent medicine physician, a physician assistant, and a psychologist. The clinic, which opened in 2011, primarily serves youth 14 and younger.
Prospective patients of the GDAAY clinic must be referred by a health care professional such as a family doctor. GDAAY’s referral form includes a question about whether it is “safe” to send correspondence to the prospective patient’s home address or home telephone number. Another question asks if there is anyone in the youth’s family that “cannot know about the youth’s gender identity.” This wording implies that the clinic views parents and family members as potential enemies of their child rather than as the most important guides in their lives.
The clinic’s website says that it often takes more than one appointment to be prescribed puberty blockers and cross-sex hormones. A physical examination and blood work may also be required before they will proceed with a hormonal transition. GDAAY also notes that, while gender surgeries are “often” performed in adulthood, adolescents aged 16 and older may get “top surgery” and adolescents aged 18 and older may receive “bottom surgeries.” The age of majority in Manitoba is 18 years old.
Another provider of a medical transition is the Trans Health Klinic, which serves adolescents aged 15 and older. In their description of their care process, they mention that hormones are dispensed on the second appointment with a medical professional. It is troubling that there seems to be no waiting period to allow other issues (e.g. mental health challenges or physical co-morbidities) to be addressed.
Psychologists at the Trans Health Clinic advertise that they write letters of recommendation for gender surgery after completing a 10–16-page assessment of gender dysphoric adolescents. This assessment for surgical readiness is based on the activist WPATH Standards of Care 8 guidelines. However, the clinic explicitly says that mental health challenges do not preclude sex-denying surgeries. The clinic does not appear to require these challenges to be explored or addressed prior to surgery.
Currently, Manitoba Health requires a diagnosis of gender dysphoria to fund any gender-related surgeries. For top surgery, the province requires one letter of recommendations (from either a health care provider or a psychologist). For bottom surgery, two recommendations are required (one from a health care provider and one from a psychologist).
Of these surgeries, Manitoba funds top surgeries (e.g. breast augmentation, chest reductions, and mastectomies) if the proper assessment form is used. The Manitoba health care system provides orchiectomies, hysterectomies, and oophorectomies within the province. Penectomies, vulvoplasties, vaginoplasties, metoidioplasties, and phalloplasties are all performed at the Centre de Chirurgie in Montreal. All these bottom surgeries are publicly funded if the assessment form is satisfactorily completed and the patient has been on cross-sex hormones for at least six months.
Prevalence
Let Kids Be filed an access to information request on any data related to gender surgeries, hormonal transitions, and visits to specialized gender clinics by minors in Manitoba. The government responded that they have no data on hormonal transitions and required an excessively high fee to collect and release surgical data. However, it did release data on the number of patient visits to the GDAAY clinic, one of the two main gender clinics in the province.
That data is summarized in the chart below. Unfortunately, the released data does not elaborate on what the abbreviations in this chart mean. Presumably, “endo” stands for endocrinologists, “SW” stands for social workers, and “PA” for physician assistants. All three are staff positions mentioned as part of GDAAY’s interdisciplinary team. It is unclear what “MH” stands for (it could be Manitoba Health, mental health, or something else).
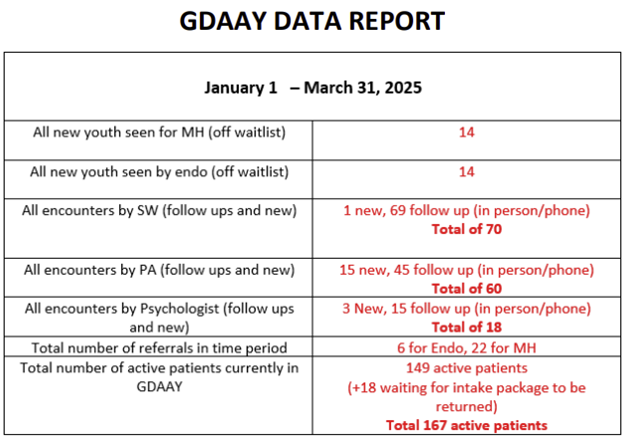
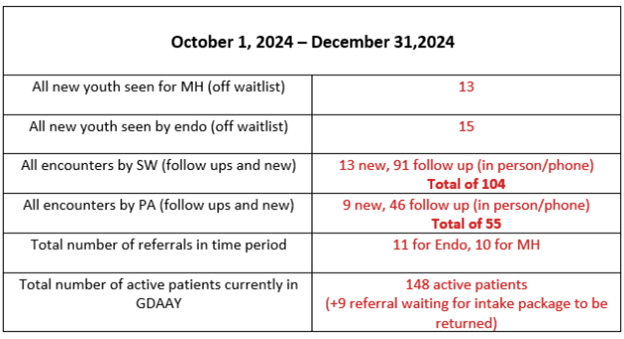
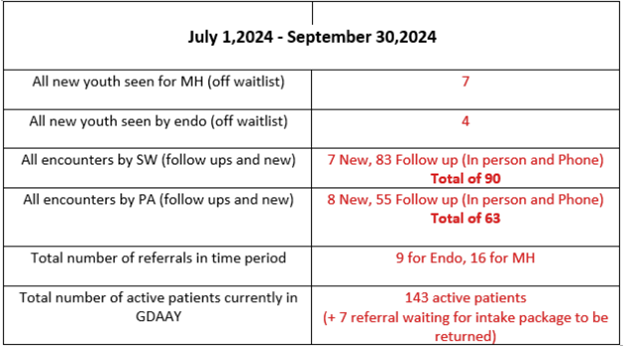
A few things stand out from this data. First, GDAAY had a slightly increasing number of active patients per quarter: from 143 in Q3 of 2024, to 148 in Q4 of 2024, to 149 in Q1 of 2025.
Second, the number of new patients also increased each quarter over the same period, from 7 to 13 to 14. That means GDAAY was on track to see 40-50 new patients in 2025. That is slightly down from the 75 new patients per year reported in 2023.
Third, a fluctuating number of youth were newly referred to or seen by an endocrinologist, with anywhere between 4 and 15 in each quarter. We do not know how many of the new patients seen by GDAAY endocrinologists were prescribed puberty blockers or cross-sex hormones. But, there would be no point in meeting with an endocrinologist if the youth did not desire a hormonal transition.
Fourth, however you look at the data, it seems that nearly all of the new youth seen at the GDAAY clinic proceeded towards hormonal transitioning. Between the three quarters, the clinic had 30 new “MH” patients, 35 new encounters with social workers, and 32 new encounters with physicians’ assistants. Thirty-three youth saw an endocrinologist. These are all likely the same patients using the services of various types of staff, and different stages of the intake process that these patients visited these professionals, likely account for the slight variation in the number of new visits here.
It clearly is not just a small fraction of gender dysphoric children visiting the clinic who are considering medical transitioning. It appears most meet with an endocrinologist to talk about it.
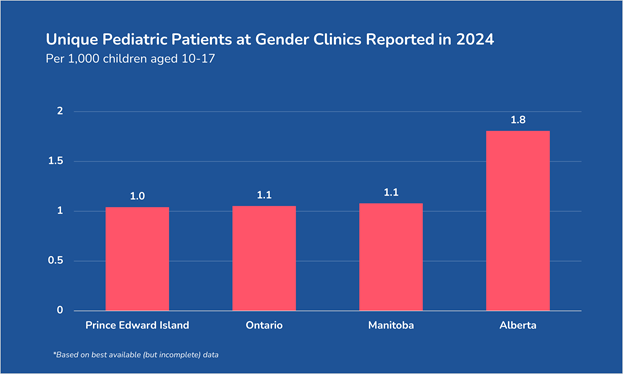
Fifth, the number of active patients seen by the GDAAY clinic translates into a comparable rate of per capita medical gender transitioning for other provinces for which data is available. We caution against making definitive comparisons between these provinces, as each has released varying amounts of data. (For example, Manitoba only reported pediatric gender clinic data for one of its two major gender clinics and for only part of the year.) But the incomplete data released by each province thus far shows a similar rate of children and adolescents visiting gender clinics.
Conclusion
Manitoba follows the crowd of Canadian provinces in pediatric gender medicine. Two clinics, GDAAY and Trans Health Klinic, are responsible for most medical transitioning for minors. Cross-sex hormones and puberty blockers are generally prescribed free of charge to children and adolescents of any age. Adolescents may obtain “top surgery” at age 16 and genital surgery at 18, with the provincial government paying for the procedure.
The province did not disclose the number of minors on puberty blockers or cross-sex hormones or who received a gender surgery. But, as we saw, it did release data on visits to the GDAAY clinic over three recent quarters.
GDAAY saw over 30 new patients and over 140 total patients in three quarters at the end of 2024 and beginning of 2025. Almost all of these new patients appear to be pursuing hormone treatments. The number of gender clinic visits is comparable to the rate of visits in other provinces based on the limited data revealed to Let Kids Be through freedom of information requests.
Liberally permitting children and teens to take puberty blockers and cross-sex hormones without any age restrictions, despite the dearth of high-quality evidence, is a travesty. Like almost every other province, Manitoba needs to put the brakes on medical gender transitioning for minors and let kids be.
In 2017, military veteran Jeff Evely took his 14-year-old daughter to the Children’s Hospital of Eastern Ontario in Ottawa to treat her depression. But last week, he was back in Ottawa to lead a coalition of de-transitioners, an advocate, a former therapist, a former school trustee, and a father, with his profound concern with gender ideology. (Gender ideology is the idea that gender, gender identity, and gender expression are disassociated with our biological sex.)
The main request in their press conference was for the federal government to repeal its conversion therapy ban so that children, adolescents, and adults alike could get counselling that would affirm their biological sex. Right now, such counselling is illegal, seen by the federal government as an attempt to “convert” someone who identifies as transgender, non-binary, or any other gender identity to identify with their natal sex.
But the unspoken petition was to ban medical gender transitioning for minors.
How did one father’s interaction with the mental health system lead to a press conference on gender ideology?
Evely, founder of Mayday, explained this journey in the press conference. Almost a decade ago, he took his then 14-year-old daughter to the Children’s Hospital of Eastern Ontario’s mental health clinic in Ottawa to manage her depression. Without his knowledge, she was transferred to the hospital’s gender clinic. The clinicians assumed that her depression, mixed with some gender atypical behaviour, must mean that a gender transition would solve her poor mental health. Evely opposed this course of action and stopped taking his daughter to the children’s hospital.
But soon, Evely was deployed abroad and unable to personally attend to his daughter’s poor mental health and gender uncertainty. While on deployment, his daughter turned 16, the legal age of medical consent in Ontario. The gender clinic then considered it fair game to start calling his daughter and to start a medical transition, despite the wishes of her father. The clinician quickly offered her puberty blockers.
Alarmed by the prospect of his daughter medically transitioning, Evely took an early leave from his tour to attend his daughter’s medical appointments.
Over the next few appointments with various health care professionals, some of which he recorded, Evely asked what evidence supported their diagnosis of gender dysphoria and their prescription of a medical transition. According to Evely, one clinician confessed that “he had absolutely no evidence whatsoever to support his assessment, but that he looked into his daughter’s heart and soul to determine that she was actually a male.” An endocrinologist said that his daughter “would commit suicide if I [Evely] didn’t support her transition, that adolescent-onset dysphoria does not desist, and that puberty blockers were completely reversible.” When he asked about the evidence to support these extraordinary claims, she responded, “we’re not going to be able to give you that evidence.”
Evely did not elaborate on whether his daughter proceeded with the medical transition or whether her gender confusion resolved naturally.
But he summed up his daughter’s personal encounter with pediatric gender medicine: “This is not medicine. It’s time for Canada to join the civilized world by banning the barbaric cultural practice of childhood medical transition.”
Next up on the speaking roster was Scott Newgent. Newgent variously self-identified as a “medically transitioned transgender adult,” a trans man, a mother, and a lesbian at various points in the press conference. Newgent is the founder of Trans Rational Educational Voices who appeared in Matt Walsh’s What is a Woman? and helped write bills in the US to ban medical gender transitioning for minors.
Newgent has personal skin in the game, living “through something I would not wish upon any child in this nation or any other: medical transition.”
“We cannot change our sex and medical transition cures nothing,” Newgent insisted. Medical transitioning is not caring, compassionate, or just. Newgent imagines a world in which children aren’t stuffed into neat gender stereotypes and are assumed to be a different gender if they don’t precisely follow these stereotypes.
Because conceiving of gender in this way – and taking it down its logical road of a medical gender transition – has many costs. The cost of medical transitioning is more than just money paid to medical professionals. The cost is in lives and in preventing children from growing up to “be who they were meant to be,” Newgent said. Newgent didn’t explicitly say what children are meant to be, but the implication is obvious: boys are meant to grow up into men and girls into women. Medical gender transitioning profoundly interferes with this development.
If an adult could be convinced of the lie of gender ideology, Newgent argued, then what chance do children have? A medical transition didn’t help Newgent. Instead, it created lifelong struggles with chronic infections, vitamin deficiencies, pulmonary embolisms, heart disease, and shortened life expectancy. This is a personal testimony of how “gender-affirming care” is anything but caring.
Drawing from Newgent’s own nightmare of medically transitioning, Newgent ended by challenging Canada to stand against medical gender transitions. “Are you willing to stand today so that a generation of children may stand unbroken tomorrow? Are you willing to take the heat today so that a child does not bear the consequences forever?” Children “deserve truth. They deserve protection. They deserve a future.”
Faith Groleau, a 26-year-old woman, provided a third personal testimony of the dangers of medical transitioning. She described being born with a hole in her diaphragm that required extensive surgery as a newborn to fix. At the age of two, she was sexually assaulted. That assault broke her collarbone, reopened that diaphragmatic hole, and rammed much of her intestines further up into her chest cavity. These internal wounds affected her health for most of her childhood but were misdiagnosed as mere asthma. These physical issues also left her in poor emotional and mental health.
Eventually, the same hospital that provided the life-saving surgery as a baby suggested that she medically transition as the fix. “A pediatrician overrode a psychiatric diagnosis – several of them,” she explained, to clear her for a medical transition. “Instead of assessing my mental health thoroughly, they decided to assume in the emergency room that my suicidal ideation came from the gender confusion. It did not. It was already there long before.” And yet, the medical professionals used this fiction to fast-track her medical transition, giving her hormones at the age of 16 and approving her for top surgery at 18.
Faith had further indictments against the team that pushed her to medically transition. “As a minor, I was emotionally groomed to manipulate my mother to tell her that, if I didn’t receive drugs or surgeries, I would kill myself. But that was not true.” Her suicidality long preceded any gender dysphoria. Beyond that, she claims that medical professionals mischaracterized the effects of drugs.
Faith explained that she was trans-identified from 16 to 24 but stopped cross-sex hormones at age 22. The withdrawal was brutal, but no medical help was offered.
“Everything that had happened to me was wrong and had nothing to do with evidence-based medicine,” she accused. (You can hear both fury and sorrow in her voice during the entirety of her remarks.) “I was experimented on. I was not told they were experimental. I was told it was medicine and that it would help. And it did none of that. It gave me complications that the doctors ignored or would treat as separate illnesses. It made my already pre-existing mental health worse. And my physical health continued to deteriorate.”
“These people do not know what they are signing up for because they are children,” she continued. “I was a child. I wanted help. That’s all I wanted. I did not need to be medicalized. I did not need to be cut up. I did not need to be drugged. I just wanted to be loved the way I was.”
Faith is currently suing the College of Physicians for malpractice, but the College maintains that the doctors did nothing wrong.
In contrast to these three intensely personal stories, Mia Hughes, a senior fellow at the McDonald-Laurier Institute and the Director of Genspect Canada, came armed with the academic evidence that Let Kids Be has been repeating for the past couple of years.
“Without any clear diagnosis, clinicians are halting the natural puberty of healthy young people, administering irreversible cross-sex hormones, and even surgically removing healthy organs, all long before these youth can possibly comprehend the life-long consequences,” Hughes claimed. She highlighted the low quality of evidence to support medical gender transitioning for minors and how this approach carries real lifelong risks. She pointed to how the UK, Sweden, Finland, Denmark, Norway, France, Italy, New Zealand, Queensland, 27 American states, and Alberta have limited hormonal transitioning. And she called out the World Professional Association for Transgender Health (WPATH) standards as “lacking developmental rigour.”
“The truth is we are witnesses of a reckless medical experiment on distressed young people, many of whom have simply misinterpreted their normal pubertal woes for a sign they are transgender,” she concluded. “The time for looking the other way is over. Indeed, the very fact that we looked away for so long is a national disgrace.”
Hughes opined that the medical professionals won’t self-correct. Governments must step in. She explicitly asked the federal government to review the evidence behind medical gender transitioning and repeal their conversion therapy ban “before more innocent youths are harmed.” But again, the unspoken ask was to ban medical gender transitioning for minors.
Three others offered very brief comments to show their support. There was Kellie-Lynn Pirie, a detransitioner and founder of the Detrans Alliance Canada. Dr. Ann Gilles lent her support as a former therapist and pastor. And Barry Neufeld, the former Chilliwack school trustee who was fined $750,000 by the BC Human Rights Tribunal for speaking out against gender ideology, also spoke up.
We applaud all seven at the press conference for their courage to stand up against gender ideology and call for an end to the federal government’s ban on conversion therapy. Just as important would have been to ask the federal government to ban medical gender transitioning for minors. Both changes – repealing Canada’s conversion therapy law and banning medical transitioning for minors – are indispensable steps to let kids be.
New Brunswick is the last stop on our tour of the Atlantic provinces’ gender medicine programs. Although these provinces aren’t known to be bastions of progressive politics (or medicine), Nova Scotia, Prince Edward Island, and Newfoundland and Labrador have all fully embraced the “gender-affirming” model of care. Nova Scotia has so bought into this gender ideology that it is one of the few provinces to confirm it has performed sex-denying mastectomies on minors. The province even green lights sex-denying genital surgeries for minors.
Is New Brunswick any better than its Atlantic peers on limiting medical gender transitioning for minors?
Sadly not.
Policy
New Brunswick is the only province in Atlantic Canada without a specialized gender clinic. Pediatric gender medicine is largely provided by the Horizon Health Network and Vitalité Health Network. These networks employ “health care professionals with specialized training in developmental processes, puberty and physical development, evolving identity exploration, legal and social transition challenges, parental and caregiver involvement, and the impact of peer, school, and community environments” to help minors transition. Alternatively, gender dysphoric children can see a pediatrician or a specialized mental health professional.
Hormone therapy is usually provided through primary care providers, pediatricians, and endocrinologists. Some of these health care practitioners may require a hormone readiness assessment letter from a medical health professional. These referral letters will generally contain any relevant diagnoses, any treatment history, and a statement of informed consent from the patient.
Horizon Health Network provides a comprehensive list of health care providers across the province involved in gender medicine. Any hormone readiness letter provided by a member of the Horizon Health Network is covered by the provincial Medicare plan, but readiness letters provided by health care professionals outside the Network typically must be paid for out of pocket.
While the government webpage on “gender-affirming care” states that their Medicare program does not cover prescription medication (such as puberty blockers and cross-sex hormones), their drug insurance plan covers many medications. New Brunswick’s Drug Plan Formulary does include the most common forms of puberty blockers and cross-sex hormones, and so the cost of most drugs used in a gender transition are paid for by the province.
To get a gender surgery in New Brunswick, a patient needs two documents: a completed Medicare Prior Approval Form and at least one referral to a surgeon. For “top surgery”, one referral letter is sufficient. For “bottom surgery”, two referral letters are required. These documents must be signed by a physician, nurse practitioner, or mental health provider who is trained in gender medicine.
The Medicare Prior Approval Form requires that the patient be at least 16 for a mastectomy and 18 for any other surgery. These age thresholds are not legislated but established by regulation by the Ministry of Health or adopted by the provincial college of surgeons.
These ages, however, are lower than the age of majority. Since the age of majority in New Brunswick is 19, this surgical requestion form explicitly allows removing the healthy breasts and reproductive organs of minors.
The Form also requires a health care professional to attest that the patient has the following:
- Persistent, well-documented gender dysphoria diagnosis
- Capacity to make a fully informed decision and to consent for treatment
- Understands the procedure(s)
- Understands associated risk(s) and complications
- Understands the effect of gender-affirming treatment on reproduction
- Reasonably well controlled medical or mental health concerns, if they are present
- Considered the role of social transition
- An aftercare / follow-up plan
For breast augmentation and genital surgery, 6 continuous months of hormone therapy is required “before the patient undergoes irreversible surgical intervention” unless patient does not wish to undertake hormone therapy.
New Brunswick covers the costs of all top and bottom surgeries, except breast construction/augmentation, out of the public purse. However, New Brunswick only performs mastectomies, hysterectomies, and orchiectomies – procedures that cut out breasts, uteruses, and testes – within the province. The remaining genital surgeries are performed by GRS Montreal.
Prevalence
Let Kids Be filed an access to information request for any data related to gender surgeries, hormonal transitions, and visits to specialized gender clinics by minors in New Brunswick. The government claims to have no data on the number of hormonal gender transitions or gender clinic visits. Puberty blockers and cross-sex hormones are used to treat many different conditions, and the government of New Brunswick says they do not have any data on what underlying condition these drugs were prescribed to treat.
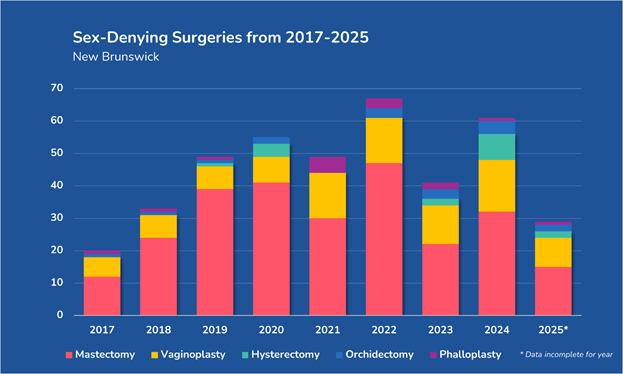
But the government did release data on sex-denying surgeries. The province found no records of any gender surgeries prior to 2015. Their records show two phalloplasties performed in 2016 (presumably in GRS Montreal). In 2017, the province began facilitating gender surgeries in earnest, though no surgeries were reported in New Brunswick hospitals that year. Presumably, all gender surgeries on New Brunswickers were performed in Quebec and Nova Scotia that year.
In 2018, New Brunswick began providing some gender surgeries (e.g. mastectomies, hysterectomies, and orchidectomies) in the province, while more complex procedures continued to be performed at GRS Montreal.
The number of gender surgeries increased quickly prior to the COVID pandemic but has fluctuated wildly since then. As we have seen in other jurisdictions, mastectomies are the most common form of gender surgeries by a wide margin, comprising 65% of all gender surgeries. Vaginoplasties were the second most common procedure, accounting for 23% of all procedures over these years.
Unlike other provinces, New Brunswick released some very interesting information: the age of the patient in each surgery. While other provinces have only given data on the number of surgeries performed on patients in big buckets (e.g. above vs below the age of majority), New Brunswick released the precise age of each patient at the time of surgery. Here is a histogram of the frequency of each type of gender surgery by patient age.
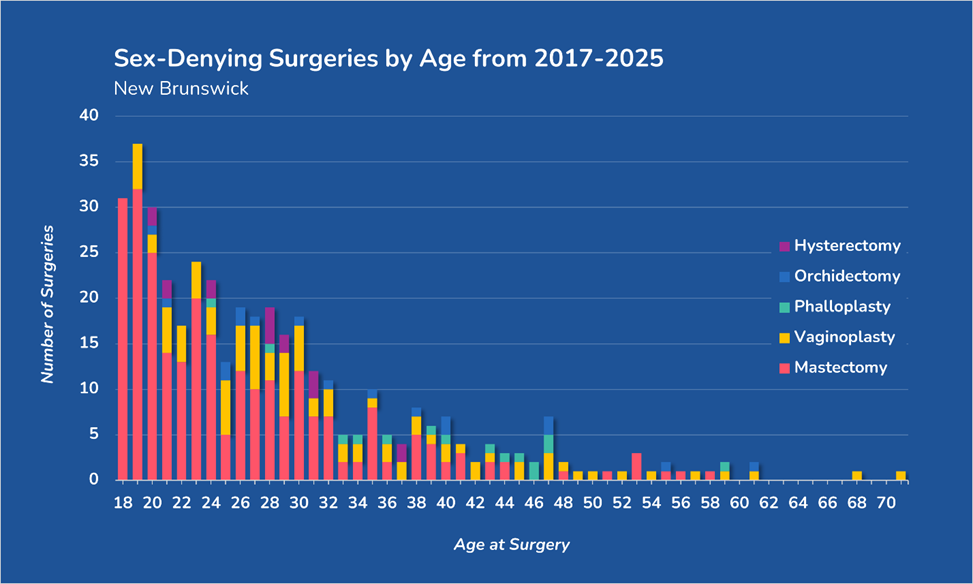
What is most noticeable in this graph is that the younger the patient, the more common surgery is. Sex-denying surgeries are most common at age 19, the age of majority in New Brunswick. Thirty-two mastectomies and five vaginoplasties have been performed on nineteen-year-olds in the past eight years.
By age twenty, young adults are starting to get hysterectomies and orchidectomies. As these surgeries remove a person’s uterus and testes, these procedures sterilize young adults for the rest of their lives.
Roughly half (48%) of all gender surgeries in New Brunswick are performed on persons at or under age 25, the age at which many scientists believe that the brain is fully developed. Almost two hundred New Brunswickers have had parts of their body amputated before their brain is fully mature.
There are also age differences in each type of sex-denying surgery. Gender dysphoric women remove female organs early in their gender transition, with the average of a mastectomy being 26 and 27 for a hysterectomy. But these women on average wait until age 41 for a phalloplasty, the attempted creation of a penis. Gender dysphoric men, on the other hand, wait on average until age 32 to get a vaginoplasty but only wait a few years longer to have their testes removed (average age of 35 for an orchidectomy).
Based on this data, gender dysphoric women are quick to get rid of their feminine organs and slow to try to ask for a penis in New Brunswick. Gender dysphoric men are the reverse. They typically ask for a vagina first and only later opt to have their male organs removed.
Conclusion
New Brunswick is a fairly typical province in Canada in its practice of gender medicine. Although it has no specialized gender clinic for either minors or adults, New Brunswick residents can still access puberty blockers and cross-sex hormones at public expense from primary care providers, pediatricians, and endocrinologists without age restriction. The health care system does limit sex-denying top surgeries to those 16 and older and bottom surgeries to those 18 and older, although this is a funding (rather than a legal) requirement.
Like most other provinces, New Brunswick was unable to provide any data on the number of children and adolescents who are hormonally transitioning. However, it provides some very unique data on the precise ages of those who received a gender surgery. These surgeries are most commonly provided to young people, with 19, 18, and 20 being the most common ages for surgery. No minors in New Brunswick received genital surgeries, but 31 received mastectomies between 2017 and 2025.
And so, just like the other Atlantic provinces, New Brunswick needs a radical policy shift to let kids be.
In 2023, Saskatchewan passed a parental bill of rights through the legislature. One of the most controversial rights in the legislation was over students’ preferred pronouns. For youth under the age of 16, the law requires schools to obtain parents’ consent before using new gendered pronouns or names. Although it drew the ire of the opposition and gender ideologues, the government even invoked the notwithstanding clause to ensure that judges could not invalidate the law.
This move required courage and resolve. We commend Saskatchewan for countering gender ideology in this manner. But has the province demonstrated any determination to protect children from medical gender transitioning?
Sadly not.
Policy
Like every other province, Saskatchewan covers the cost of puberty blockers and cross-sex hormones. If a person resides in Saskatchewan and has a Saskatchewan health card, the government generally covers the cost of these drugs.
Saskatchewan was the most hesitant of Canada’s provinces to fund sex-denying surgeries, but that isn’t saying much. It funds mastectomies and all genital surgeries. However, Saskatchewan does not pay for breast augmentation, chest contouring, facial surgery, tracheal surgery, or body contouring.
The procedures that Saskatchewan actually provides are a different story. The provincial health care system performs mastectomies (breast removals), breast augmentation, chest contouring, hysterectomies (uterus removal), oophorectomies (ovary removal), and orchiectomies (testicle removal).
Saskatchewan sends residents to GrS Montréal for any metoidioplasties and phalloplasties (surgeries to construct a simulacrum of a penis), vaginoplasties (attempts to create a vagina), and vulvoplasties (attempts to create vulva). In essence, Saskatchewan’s surgeons have the capability to cut away healthy genitals, but not to try to construct new ones.
To get a surgery in Saskatchewan, all one needs is a referral from a primary care provider.
Getting a surgery out of province is more complicated. First, a primary care provider must refer a patient to a specialist practicing in a relevant field in Saskatchewan. That specialist must write a letter to the ministry pitching the case for surgery. The Ministry of Health’s medical consultant will then assess whether the case merits public funding. If funding is granted, an applicant must still meet any requirements for surgery set by the surgeon at GrS Montréal.
Providers
Most providers of gender medicine are family doctors. TransSask, a pro-transgender non-profit, provides two “trans health navigators” to help people “those seeking gender-affirming healthcare, including hormone therapy, surgery referrals, finding an affirming doctor, and accompaniment to appointments,” but these navigators do not provide medical services themselves.
Unlike larger provinces, Saskatchewan does not have any community clinics or hospital-based programs that specialize in gender medicine. However, the Saskatoon Community Clinic provides “gender affirming care, including puberty suppression for youth.” Because it does not accept self-referrals, would-be patients must be referred by a primary care provider. The clinic advises that it generally provides a gender-affirming care appointment once every 3 months for the first year and once every 6-12 months thereafter.
Prevalence
Let Kids Be filed an access to information request on any data related to gender surgeries, hormonal transitions, and visits to specialized gender clinics by minors in Saskatchewan. The government responded that they have no data on hormonal transitions or gender clinic visits.
This dearth of data demonstrates that this isn’t even an issue on the government’s radar. A growing number of countries around the world are concerned with the ramifications of prescribing puberty blockers and cross-sex hormones to minors. This includes all of Canada’s most comparable peers: the United Kingdom, the United States, Australia, and New Zealand. But Saskatchewan has refused to acknowledge that there is any problem with stunting the sexual development of children or assisting them to develop in the opposite way that their bodies intended them to develop. And without recognizing any problem, the government hasn’t bothered to collect data on pediatric medical transitioning rates.
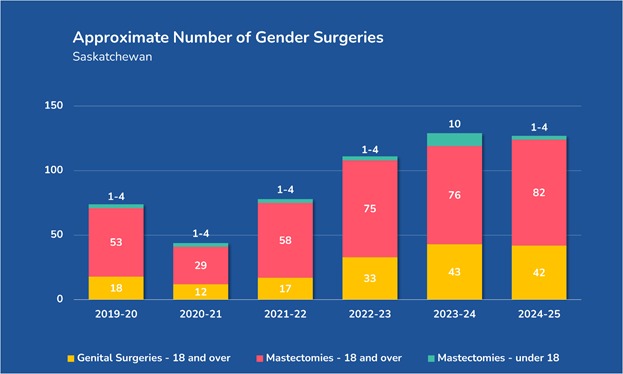
But the government was able to release some data on sex-denying surgeries over the past six years. As usual, counts less than five are redacted to preserve patient privacy.
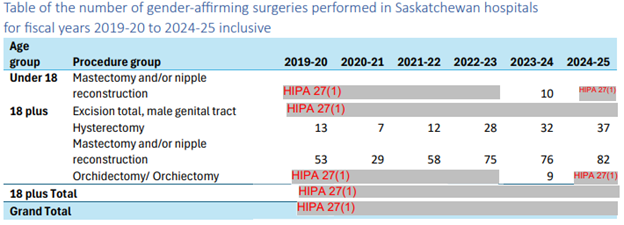
This data confirmed that many of the more complicated sex-denying surgeries are not available within Saskatchewan, but some surgeries are performed in the province. The province performed 373 mastectomies (the removal of breasts), 127 hysterectomies (the removal of the uterus), at least 14 orchidectomies (the removal of testicles), and at least 6 removals of the male genital tract on adults from 2019 to 2024.
As an aside, this date confirms yet again a gender skew. The vast majority of these surgeries – performed on both minors and adults – are attempts by women and girls to become more masculine. Saskatchewan performed at least 388 breast removals over six years. The number of breast augmentations? Zero. Similarly, at least 86% of all bottom surgeries targeted the reproductive organs of women. Some of these discrepancies may stem from Saskatchewan not funding the full gamut of gender surgeries. But, if those who identify as transgender or non-binary need these procedures as much as gender ideologues claim, surely some would have paid the cost. None show up in the data.
Sadly, although no genital surgeries were recorded for minors, at least 15 minors received mastectomies. Ten gender dysphoric adolescents lost their breasts in 2023, and at least one (but fewer than five) received a mastectomy in each of the remaining years from 2019 to 2025.
Conclusion
Despite being willing to tackle gender ideology in schools, Saskatchewan has been unwilling to address gender-ideology-driven medicine in doctors’ offices and hospitals. The province funds puberty blockers and cross-sex hormones, which are prescribed to gender dysphoric children by their family doctors. The province also pays for most sex-denying surgeries, sending patients to Quebec to receive the most complicated procedures.
Saskatchewan is the third province thus far in Canada to confirm that it provides gender surgeries for minors within its borders. Both Alberta and Nova Scotia performed “gender-affirming” mastectomies on minors in their hospitals. Ontario revealed that it sent minors out of province or out of the country for sex-denying surgeries, but did not confirm whether they performed them in-province (though they likely do). At least 15 minors received mastectomies in Saskatchewan since 2019.
As the birthplace of publicly funded health care in Canada, it is tragic to see the public health care system transition away from providing true medical care that preserves bodily integrity to promote health. Instead, Saskatchewan’s medical system is all too willing to provide gender transitions for minors.
The United Kingdom has just banned the last available facet of medical gender transitioning for minors: cross-sex hormones as a treatment for gender dysphoria for 16- and 17-year-olds. After comprehensively reviewing the evidence around cross-sex hormones for minors, the National Health Service concluded, “there is not enough evidence to support the safety or clinical effectiveness of feminising and masculinising medicines to make the treatment routinely available to children and young people at this time.”
This is but the latest development in the United Kingdom’s ongoing public policy debate about medical transitioning for minors that has led to a full ban on the practice. It’s also one that Canada should follow.
Before the Cass Report, an independent investigation into pediatric gender medicine, the United Kingdom had no firm age restrictions for puberty blockers and cross-sex hormones. The country’s Gender Identity Development Service routinely prescribed puberty blockers at the onset of puberty. Cross-sex hormones, if desired, were prescribed starting at age 16 and gender surgeries, if desired, were offered only to adults past age 18.
The interim Cass Review in February 2022 and the final Cass Review in April 2024 questioned this approach, citing the lack of evidence to support these medical transitions. The government responded to puberty blockers and cross-sex hormones separately.
Regarding puberty blockers, the government issued a temporary three-month ban on using these drugs to treat gender dysphoria in May 2024. This temporary ban was extended in August and then in November before the government made the ban on puberty blockers indefinite in December. The only exceptions to this ban were for those already on puberty-blockers or those enrolled in the upcoming PATHWAYS clinical trial.
The PATHWAYS trial was designed to study how puberty blockers would impact the physical, social, and emotional well-being of children with gender dysphoria. Since all the evidence around puberty blockers to treat gender dysphoria was of low quality or low certainty, the UK planned a study to yield high-quality and high-certainty evidence. Would puberty blockers alleviate gender dysphoria? Or would they cause harm?
PATHWAYS was intended to be the first randomized controlled trial to study these outcomes. One group of gender dysphoric kids would be given puberty blockers immediately, and another group would be given puberty blockers twelve months later. The impacts of the puberty blockers would be assessed by comparing the two groups for the first twelve months (i.e. before the second group received their puberty blockers).
Although the desire for better evidence is laudable, the study design was not. Both sides of the issue argued that this study would harm children. The pro-transitioning side argued that withholding puberty blockers would harm the gender dysphoric children, forcing them to go through puberty against their will. The pro-let-kids-be side argued that giving any children puberty blockers would cause harm and that the study would only allow outcomes for the first twelve months to be collected. Fundamentally, the trial would treat children as lab rats, receiving ethically and medically dubious treatment so that the medical establishment could learn more about the effects of puberty blockers.
In response to these criticisms, the government announced in February 2026 that the PATHWAYS trial would be paused until these concerns could be resolved.
On the cross-sex hormone front, the UK government initially restricted cross-sex hormones to those over the age of 16 in June 2023. Although they explored whether it would be appropriate to allow children under 16 to take cross-sex hormones, the government reiterated in March 2024 that 16 should be the minimum age to receive cross-sex hormones. Persistent gender dysphoria was then a prerequisite, and a multi-disciplinary team had to endorse a referral for cross-sex hormones for 16- and 17-year-olds.
But the government’s latest decision on March 9, 2026, raises the floor even further, banning new prescriptions for cross-sex hormones for 16- and 17-year-olds. However, the National Health Service has opened up a 90-day consultation period to see if there is any evidence, impacts, or policy alternatives that they might have missed. The feedback on this policy could still lead to another policy revision this summer. But given the rigorous review the UK has already undertaken on the evidence regarding cross-sex hormones for minors, it would take significant new information for them to change their policy.
All of this stands in stark contrast to the approach to medical transitioning in Canada. Only Alberta bans all forms of medical transitioning below the age of 16 and only allows 16- and 17-year-olds to access puberty blockers and cross-sex hormones with parental, physician and psychologist approval. Every other Canadian province has ignored the growing consensus that little high-quality evidence supports medical transitioning for minors.
That needs to change. Every Canadian province needs to get serious about critically evaluating “gender-affirming care” and consider severely restricting these interventions.
On February 3rd, the Society issued a new position statement on gender surgery for children and adolescents. It’s nine pages long, but here is the main point:
“[Given] the overall evidence base for gender-related endocrine and surgical interventions is low certainty, and in light of recent publications reporting very low/low certainty of evidence regarding mental health outcomes, along with emerging concerns about potential long-term harms and the irreversible nature of surgical interventions in a developmentally vulnerable population, ASPS concludes there is insufficient evidence demonstrating a favorable risk-benefit ratio for the pathway of gender-related endocrine and surgical interventions in children and adolescents. ASPS recommends that surgeons delay gender-related breast/chest, genital, and facial surgery until a patient is at least 19 years old.“
Let’s break it down.
The ASPS recognizes that there isn’t much certainty around the outcomes of medically transitioning minors. It repeatedly cites the United Kingdom’s Cass Review and the United States’ Treatment for Pediatric Gender Dysphoria: Review of Evidence and Best Practices. One of the central findings of both reports, which reviewed all the available evidence, was that there is simply little to no high-quality evidence to assess medical transitioning for minors. What evidence is out there is of low certainty because of small sample sizes, bias, and other methodological errors
The plastic surgeons’ society also notes the long-term harms and irreversible nature of medical transitions. Of course, these are even more immediate with surgeries than with puberty blockers or cross-sex hormones. These surgeries remove healthy organs. Mastectomies cut away breasts. Hysterectomies remove the uterus. Orchidectomies destroy testes. Penectomies chop off penises. There is no way to replace these intricate organs. Plastic surgeons can insert prosthetics or graft skin to create structures that look like breasts or a penis, but they cannot function. These surgeries are irreversible.
The ASPS statement also mentions that minors are developmentally vulnerable. In other words, their brain and body are still developing. Most physical development continues into mid- to late-teens, but the brain isn’t fully mature until around age 25. Apart from physical developments, the position statement notes that a teenager’s identity development is complex and long-term. The body, the brain, and identity are all in flux during adolescence and childhood.
The harms of gender surgeries often outweigh the benefits for minors. The position statement notes that the “available evidence suggests that a substantial proportion of children with prepubertal onset gender dysphoria experience resolution or significant reduction of distress by the time they reach adulthood, absent medical or surgical intervention.” As we’ve noted elsewhere, that figure is 80-90%. Thus, most children and adolescents will obtain the desired benefit of surgery – alleviation of gender dysphoria – without undergoing surgery at all.
Now, some gender ideologues may object that gender surgeries are about more than treating gender dysphoria. Gender dysphoria aside, a person may have “embodiment goals” related to their gender identity, and they might demand that doctors help them achieve these goals.
But the American Society of Plastic Surgeons’ position statement addresses this argument. “Patient autonomy is more properly defined as the right of a patient to accept or refuse appropriate treatment; it does not create an obligation for a physician to provide interventions in the absence of a favorable risk–benefit profile, particularly in adolescent populations where decision-making capabilities are still developing. In pediatric contexts, the threshold for intervention must be higher and safeguards more stringent.”
In other words, patient autonomy means doctors can’t force a patient to undergo a particular treatment. It does not mean that patients are entitled to whatever surgery they want. Unfortunately, that is what gender medicine has become. Doctors have become vending machines for puberty suppressants, hormones, and surgeries.
Given all that is known about gender surgeries, the ASPS recommends that no surgeon provide a gender surgery for anyone under 19.
The Association’s recommendation likely isn’t binding. If a plastic surgeon does a gender surgery on a minor in the United States, they likely won’t get in trouble with the ASPS. It only recommends not doing such surgeries, after all.
It’s a step that the Canadian Society of Plastic Surgeons still refuses to follow, though it did commit to taking a closer look at the evidence and publishing a formal position. In response to the ASPS’s lengthy position statement, the CSPS issued the following statement:
“The Canadian Society of Plastic Surgeons (CSPS) is aware of the recent position statement issued by the American Society of Plastic Surgeons (ASPS) regarding gender surgery for children and adolescents.
At present, the CSPS does not have a formal position statement on this issue. The CSPS respects the physician-patient relationship and supports the role of individual surgeons in providing care that is appropriate and ethical.
The CSPS is committed to clinical decision-making focused on evidence-based medicine such as, in this area of practice, information provided by the World Professional Association for Transgender Health (WPATH).
The CSPS plans to establish a working group of Canadian plastic surgeons with expertise in this area to review the evidence and assist in the preparation of a more formal position. The CSPS remains committed to supporting its members as they navigate complex and evolving areas of practice.”
The problem, of course, is that WPATH’s guidance is not evidence-based, as the CSPS statement implies. South of the border, the American Society of Plastic Surgeons isn’t alone in recognizing this. Soon after the ASPS released its position statement, the American Medical Association voiced its support for reserving any sex-denying surgeries until adulthood.
But that’s not the end of the recent news.
Jury finds medical malpractice in medical transitioning suit
Just a week earlier, a jury awarded a woman who had a double mastectomy in her teens a $2 million award against her surgeon and psychologist for medical malpractice in the case of Varian v. Einhorn.
The details of the case are scarce as the court documents are sealed (i.e. unavailable to the public). What is known is that the plaintiff in the case, Fox Varian, struggled with her identity as a woman beginning at age 15. She began binding her breasts, changed her name, and began publicly identifying herself as a man. She visited a psychologist – the Kenneth Einhorn named in the case – for help with her medical transition, though he had no formal training in transgender-related health care. He suggested puberty blockers as the first stop in her transition, but Varian wanted a top surgery. And so, nine months after first expressing her desire to surgically transition, Einhorn referred her for surgery.
However, Einhorn never diagnosed Varian with gender dysphoria, the prerequisite for a “gender-affirming” surgery according to WPATH’s standards of care. Instead, he diagnosed her with body dysmorphia, a fixation on a perceived flaw in one’s appearance. He wrote a referral for surgery despite Varian having confided in another counsellor that she was still unsure of her gender identity. Einhorn had recommended this counsellor – or at least their organization – but never bothered to communicate with this counsellor about what these counselling sessions revealed.
Einhorn also presented a classic line of argument to Varian’s mother, Claire: if Varian didn’t medically transition and get an “affirming” mastectomy, she was at risk of committing suicide. At first, Claire opposed the idea, but the psychologist was persistent and insistent. Eventually, in what was “the hardest, most difficult, gut-wrenching” decision, Claire (and presumably Varian) consented to the double mastectomy. However, they were never informed of the “the risks, hazards, and alternatives” of the surgery and her “other psychological conditions, including anorexia, depression, ADHD, autism, and body dysmorphia” were not properly addressed prior to the surgery.
And so Vivian underwent the gender surgery at the age of 16.
It didn’t take long for her to realize her mistake. She detransitioned and launched a lawsuit against both her psychologist and her surgeon, charging that they failed to obtain fully informed consent for the surgery. And this year, at the age of 22, a jury agreed and awarded her $2 million in damages.
Although there are many more such cases in the works, this is the first case in which a detransitioner successfully sued health care professionals who facilitated a hasty medical transition. It likely won’t be the last.
With the American federal government opposed to the practice, courts upholding state bans, medical professional bodies recommending against pediatric surgeries, and now health professionals being sued over these procedures, medical transitioning for minors is increasingly restricted in the United States.
Those minors are finally getting the protections that they need south of the border. Now Canada needs to follow suit.
Seven hundred and seven days after Alberta Premier Danielle Smith announced that Alberta intended to protect minors from medical transitioning, the province has fully implemented that commitment. Alberta now fully bans sex-denying surgeries for minors. Albertans under 16 may not be given puberty blockers or cross-sex hormones, unless they already started taking them. Sixteen- and seventeen-year-olds can access puberty blockers and cross-sex hormones with parental, physician and psychologist approval.
This is a huge triumph! Alberta is the first province in Canada to legally restrict these harmful interventions.
But it wasn’t an easy path to get here. After many legislative hurdles and judicial interventions, let’s chronicle how this came to be.
January 31, 2024 – Danielle Smith announces on social media her government’s plan to restrict medical transitioning for minors, require parental notification or permission for a child to socially transition at school, and preserve women’s-only sports. This announcement came as a surprise as it was not part of the United Conservative Party’s election platform.
October 31, 2024 – The main piece of legislation to ban medical transitioning for minors, Bill 26: Health Statutes Amendment Act, 2024 (No.2), was introduced in the Alberta legislature. The bill contained three important clauses. Section 1.91 prohibits sex-denying surgeries for all minors. Section 1.92 prohibits puberty blockers or cross-sex hormones for all minors under 18, though Section 1.93 allows the Minister of Health to create exceptions.
December 5, 2024 – Bill 26 receives royal assent. The prohibition on sex-denying surgeries for minors goes into effect immediately, but the sections dealing with puberty blockers and cross-sex hormones do not. The government claims that the ban on puberty blockers and cross-sex hormones will come into effect once the Minister of Health crafts and signs a ministerial order allowing mature minors and those already on these drugs to access them.
July 27, 2025 – Justice Allison G. Kuntz issues an injunction preventing the ban on puberty blockers and cross-sex hormones from going into effect. Various pro-LGBTQ organizations, parents, and children challenged the legislation in court. Justice Kuntz opined that this ban on puberty blockers and cross-sex hormones might infringe on the Charter right to equality and to life, liberty, and security of the person. Until these rights can be considered in full in a future case, she temporarily blocked the ban on hormonal transitioning from going into effect. The ban on sex-denying surgeries was left unchallenged and remained in force.
September 8, 2025 – Health Minister Adriana LaGrange creates exceptions for the blanket ban on puberty blockers and cross-sex hormones for minors in Ministerial Order 31/2025. These exceptions allow minors who had already started these hormonal interventions or started these interventions in another province to continue to receive these drugs. The order also allows mature minors aged 16 and 17 to access puberty blockers and cross-sex hormones with parental, physician, and psychologist approval. It also exempts children with an intersex condition who also experience gender dysphoria.
November 18, 2025 – The Alberta government invokes the notwithstanding clause in Bill 9: Protecting Alberta’s Children Statutes Amendment Act, 2025. The notwithstanding clause is a constitutional provision that allows laws passed by the elected legislature to remain constitutional notwithstanding the decisions of appointed courts. However, the constitution stipulates that the notwithstanding clause expires every five years unless renewed by another act of the legislature.
December 11, 2025 – Bill 9 receives royal assent. This law nullifies Justice Kuntz’ injunction preventing the ban on hormonal transition from coming into effect and paves the way for the full set of restrictions on medical transitioning for minors to come into force. It also prevents any future court decisions from striking down the restrictions.
January 7, 2026 – Alberta brings the ban on puberty blockers and cross-sex hormones into effect. It is now illegal to prescribe puberty blockers or cross sex hormones to minors to treat gender dysphoria, with exceptions for mature minors, those who were already on these hormones, and those with an intersex condition.
This brings us up to the present. But that is by no means the end of the story.
The government is still appealing the temporary injunction against the ban on hormonal transitioning by Justice Kuntz. Furthermore, Egale and company are still waiting for the court to officially opine on whether the ban violates the Charter of Rights and Freedoms. In some ways, the outcomes of these two cases don’t matter. Even if the judges find the ban violates certain sections of the Charter, the ban is saved by the notwithstanding clause of the Charter. However, a ruling by the courts that the ban on medical transitioning for minors does violate the Charter rights of gender dysphoric children will likely sap public support for the ban.
Also, the notwithstanding clause protecting this ban expires on December 11, 2030, unless it is renewed by the government. If the clause is allowed to expire and if the courts rule that the ban on medical transitioning is unconstitutional, then gender dysphoric children will again be at risk of the harmful and potentially irreversible consequences of gender medicine.
But until then, Alberta is leading the way in Canada in letting kids be.
Each of Canada’s ten provinces regulates gender medicine differently. This gives each province the ability to adapt to new evidence more quickly and respond to the demands of local citizens better than if health care were centralized with the federal government. But this also means that it is harder to understand all the nuances of each system and to collect data from across the country. Over the coming months, we will do our best to profile the data and policies on medical transitioning for minors in each province.
Newfoundland and Labrador is unique. It was the last province to join Canada (in 1949), has its own special time zone (30 minutes ahead of the rest of Atlantic Canada), and boasts the most distinctive accent in the country. The population of the entire province is smaller than the city of Hamilton, Surrey, or Quebec City. It is the least densely populated province in Canada, and just under half of the population resides in or around St. John’s.
Unfortunately, Newfoundland and Labrador is not unique when it comes to sex-denying medicine. While it does not perform sex-denying surgeries due to its size and lack of facilities, the province has not tapped the brakes on medical transitioning for minors.
Policy
Newfoundland and Labrador’s Medical Care Plan (MCP) generally covers the cost of puberty blockers and cross-sex hormones. The public health system also covers the cost of most sex-denying surgeries, but not all (e.g. facial feminization or voice pitch surgery).
Notably, all of the province’s policies and procedures relating to medical transitioning are based on the seventh version of WPATH’s Standards of Care (released in 2012) rather than the eighth version (released in 2022). The older edition notes that only 6-23% of cases of gender dysphoria in prepubertal children persisted into adulthood. Thus, “in most children, gender dysphoria will disappear before or early in puberty.”
Given this reality, the Standards of Care 7 are a bit more cautious about “gender-affirming care.” They recommend that clinicians working with gender dysphoric children and adolescents provide “supportive psychotherapy to assist children and adolescents with exploring their gender identity, alleviating distress related to their gender dysphoria.” But the Standards still support sex-denying procedures.
The seventh edition of the Standards of Care requires four criteria to be satisfied for clinicians to provide puberty blockers:
- The adolescent has demonstrated a long-lasting and intense pattern of gender nonconformity or gender dysphoria;
- Gender dysphoria emerged or worsened with the onset of puberty;
- Any co-existing psychological, medical, or social problems that could interfere with treatment have been addressed;
- The adolescent has given informed consent and, particularly when the adolescent has not reached the age of medical consent, the parents or other caretakers or guardians have consented to the treatment.
The Standards give no requirements for cross-sex hormones for minors specifically, though the following criteria are for hormone therapy in general:
- Persistent, well-documented gender dysphoria;
- Capacity to make a fully informed decision and to consent for treatment;
- Age of majority in a given country (if younger, follow the Standards of Care outlined in section VI [on children and youth]);
- If significant medical or mental health concerns are present, they must be reasonably well-controlled.
Curiously, although the third criterion refers to the section on children and youth, the section provides no further guidance on the prescription of cross-sex hormones to minors.
The Standards of Care 7 recommend that genital surgery not be performed prior to the age of majority, but suggests doing mastectomies earlier, “preferably after ample time of living in the desired gender role and after one year of testosterone treatment.” The requirements for surgery are the same as for cross-sex hormones, with the additional requirements of “12 continuous months of hormone therapy as appropriate to the patient’s gender goals (unless the patient has a medical contraindication or is otherwise unable or unwilling to take hormones)” for all genital surgeries and a further requirement of “12 continuous months of living in a gender role that is congruent with their gender identity” for genital reconstruction surgeries.
Thus, these requirements mandate no hard age limits on medical transitioning for minors, with the exception that bottom surgery is not recommended before the age of majority.
Providers
Trans Support NL, a non-profit organization that receives government funding, states that most gender-affirming care in the province is provided by a small group of providers that are mostly based in the St. John’s area. In response, the province is working to train primary care providers to provide gender-affirming care themselves. On its medical transitioning page, Trans Support NL encourages anyone seeking hormone replacement therapy to contact their family doctor.
However, there is one pediatric Gender Wellness Clinic at the Janeway Children’s Health and Rehabilitation Centre in St. John’s. The clinic serves children and youth under the age of 18 and is staffed by pediatric endocrinologists who prescribe puberty blockers and cross-sex hormones.
According to WPATH’s Standards of Care 7, only health care providers who meet “WPATH credentials” may provide surgical readiness assessments. Trans Support NL’s website lists four doctors who provide such assessments, though they note that the list is not exhaustive. Previously, the province had required a referral from the Centre for Addiction and Mental Health in Toronto for surgery.
The province does not perform most gender surgeries within the province. Most “top” surgeries are performed in New Brunswick, while most genital surgeries are performed at GRS Montreal.
Prevalence
In response to an access to information request, the government of Newfoundland and Labrador did not have any records detailing the number of minors who had received sex-denying interventions. The province was able to release data on the number of patients of all ages receiving puberty blockers or cross-sex hormones, but only for all underlying conditions (e.g. precocious puberty, breast or prostate cancer, menopause, or naturally low hormone levels in addition to a medical transition).
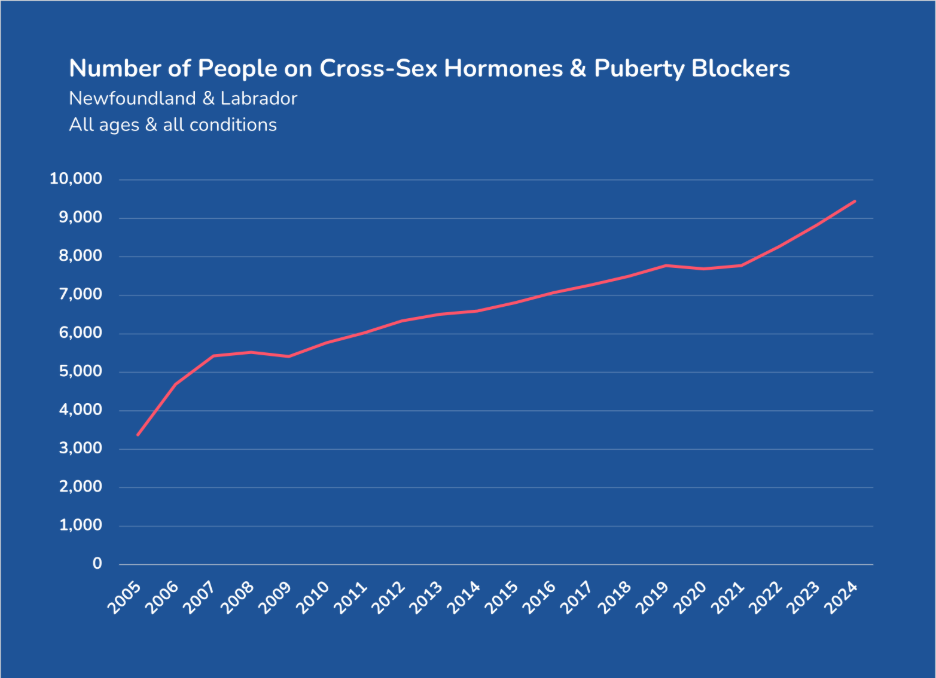
Given this level of aggregation, it is impossible to deduce the number of children, adolescents, or even adults who are hormonally transitioning. However, the use of these drugs has nearly tripled in two decades. More minors who are medically transitioning may be one factor driving that growth, but we cannot know for certain.
The only surgical data that Newfoundland & Labrador released was that it approved 169 sex-denying mastectomies between November 2019 and May 2022. Only 22 of these mastectomies were actually performed, however. One reason for this discrepancy could be that some women and girls reconsidered having their breasts permanently removed. The more likely reason is that, since no facility regularly performs these surgeries, most gender dysphoric women and girls have not (yet) travelled to have a mastectomy. The province provided no information regarding the age of the patients for whom mastectomies were approved or performed.
Conclusion
Although there are no legal restrictions on medical transitioning for minors in Newfoundland & Labrador, the province does rely on the older – and slightly more stringent – WPATH Standards of Care 7. These standards permit puberty blockers, cross-sex hormones, and top surgeries for minors, though they recommend bottom surgeries only after the age of majority. All of these procedures are eligible for public funding. No data on the number of minors who are medically transitioning is available.
And so, while Newfoundland & Labrador might be unique, they are not unique in their liberal provision of medical transitioning.
Each of Canada’s ten provinces regulates gender medicine differently. This gives each province the ability to adapt to new evidence more quickly and respond to the demands of local citizens better than if health care were centralized with the federal government. But this also means that it is harder to understand all the nuances of each system and to collect data from across the country. Over the coming months, we will do our best to profile the data and policies on medical transitioning for minors in each province.
Prince Edward Island is the setting for a renowned children’s story: Anne of Green Gables. In the classic tale, an imaginative, talkative, and red-haired orphan is adopted by the Cuthberts. Anne initially struggles to fit in and bucks traditional norms. Accidentally dying her hair green doesn’t help. But through growth, love, and self-sacrifice, Anne eventually settles down and gives up her educational dreams to care for her adoptive mother. These themes reflect the values and times of 1908, the date Anne of Green Gables was published.
Many girls have similar struggles about fitting into today’s society. One of those growing struggles is over what it means to be a female or whether it is even possible to define what a woman or a girl is. A girl pushing back against gendered expectations (e.g. perhaps purposely dying her hair green) today might be drawn in by trans influencers, contract gender dysphoria, and pursue a medical transition to find belonging and identity.
Sadly, rather than encouraging a modern Anne to allow time and biology to take their course, Prince Edward Island would be all too willing to help Anne medically transition.
Policy
According to PEI’s Primary Care Toolkit, the Consent to Treatment and Health Care Directives Act allows minors over the age of 16 to consent to sex-denying hormones without parental consent. No minimum ages are required or recommended for puberty suppression or hormone therapy, though states of puberty are mentioned. Puberty suppression is recommended in “the early stages of puberty” and hormone therapy for those “past puberty or well-advanced in puberty.” As with all other provinces, PEI covers the cost of puberty blockers and cross-sex hormones.
Prince Edward Island publicly funds more forms of sex-denying surgeries than any other province. In addition to paying for all forms of genital surgeries as well as both mastectomies and breast augmentations, the province will also pay for procedures that other provinces deem cosmetic or non-medically necessary. This includes facial surgery, hair removal or replacement therapy, voice therapy, and gamete harvesting and preservation.
For the province to cover the cost of these surgeries, physicians or mental health professionals who are trained in “gender-affirming care” (as defined by WPATH’s SOC 8) must assess the patient, recommend surgery, and complete a Gender Confirming Surgery Prior Approval Request Form. This form requires applicants for surgery to affirm that they are at least 18 years old. A physician must also attest to this age requirement for genital surgery further on. This seems to rule out sex-denying surgeries for minors. However, the Primary Care Toolkit notes that “there may be rare exceptions for those who began their transitions at a young age.”
Providers
The government’s Gender-Affirming Health Services page offers two different routes for a medical transition for minors. Minors under the age of 16 are directed to a pediatrician to discuss any medical transition. Those over the age of 16 are encouraged to contact their primary health provider. These pediatricians and family doctors can prescribe sex-denying hormone therapy. Alternatively, these mature minors can visit the Gender Affirming Clinic in Charlottetown, a clinic that is open on the first and third Wednesdays of each month.
Due to the province’s small population, most sex-denying surgeries are not performed on the island. Most are performed at GrS Montreal except for hysterectomies (removal of the uterus) and oophorectomies (removal of the ovaries), which are performed locally.
Prevalence
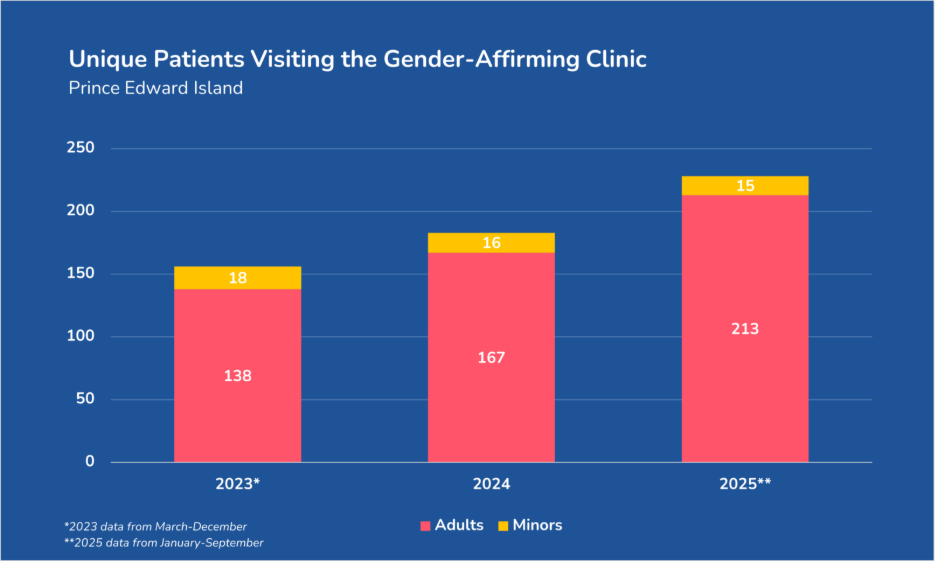
In response to our access to information request, Prince Edward Island did not have any data on the number of people who visited a primary care provider for gender dysphoria or the number of patients currently prescribed puberty blockers or cross-sex hormones. The province was only able to release the number of patient visits and the number of unique patients to the province’s one Gender-Affirming Clinic. This data covered only the last three years and does not capture all of 2023 nor all of 2025.
In each of these (partial) years, the majority of patients were adults. Despite the steady growth in the number of adults visiting the clinic, the number of minors has remained relatively stable over the past three years. At least eighteen minors visited the Gender-Affirming Clinic in the last 10 months of 2023, although a couple more may have dropped in January and February that year. Sixteen visited in 2024. Fifteen visited through the first nine months of 2025, but by the end of the year, that total will likely be a few visitors higher.
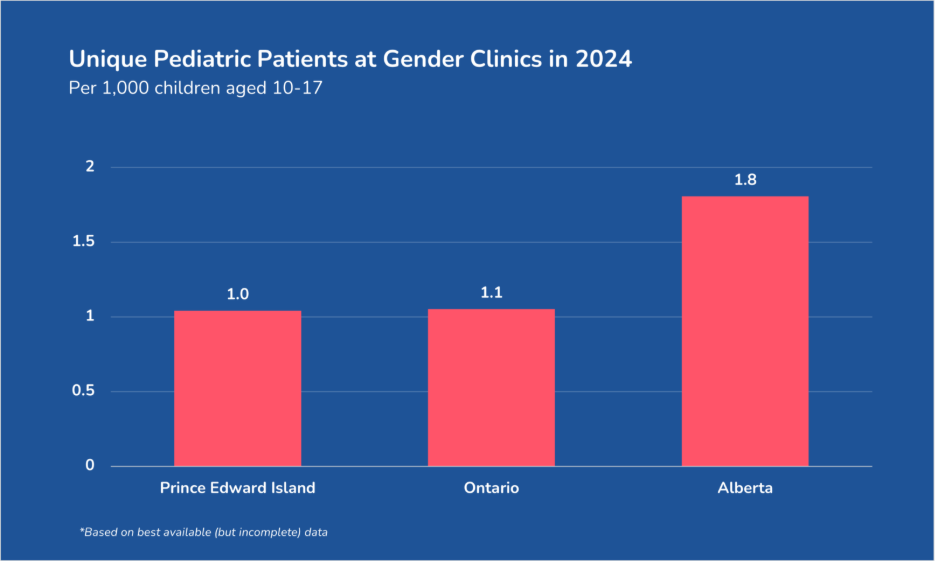
These numbers may be small, but that is because Prince Edward Island has a small population of around 182,000. (For comparison, the entire population of the island is comparable to the mid-sized cities of Sherbrook, Oshawa, or Abbotsford.) Thus far in this series, we have data on the number of unique pediatric visitors to the Gender-Affirming Clinic in Prince Edward Island, the hospital-based gender clinics in Ontario, and the hospital-based gender clinics in Alberta. If we compare the number of children and adolescents who visited these with the number of children and adolescents in each of these provinces, the rates of minors seeking help with their gender dysphoria are comparable. In Prince Edward Island, there are 1.0 pediatric gender clinic visits per 1,000 children aged 10-17. In Ontario, that rate was 1.1. In Alberta, it was 1.8. While this data is incomplete (e.g. it does not take into account community gender clinics in Ontario or Alberta), this gives us some idea of the rate at which children and adolescents are seeking help with gender dysphoria.
The province reports that fewer than five sex-denying procedures have been performed in the province in the last 25 years. Given that all other surgeries are performed out of province, these surgeries were likely hysterectomies and oophorectomies. All of these surgeries were performed on adults. No sex-denying surgeries have been performed in minors in PEI.
Conclusion
Despite its small size and population, Prince Edward Island is not immune to the promotion of medical transitioning. It fully funds more types of sex-denying procedures than any province in the country. Although gender surgeries are limited to adults, there are no age restrictions on hormonal interventions. Most children suffering from gender dysphoria are referred to pediatricians or family doctors, though there is one dedicated gender clinic in Charlottetown. Forty-nine minors have visited this clinic in the last three years, but the number of minors who have been treated for gender dysphoria by family doctors is unknown. The number of children and adolescents who are on puberty blockers and cross-sex hormones is also unknown. Thankfully, there is no record of any underage Prince Edward Islander ever receiving a sex-denying surgery.
With nearly 40% of Canada’s population, Ontario likely provides the greatest number of medical transitions to minors in the country. While the Ontario policy and providers of sex-rejecting interventions are publicly available, any specific statistics on the number of children and adolescents who are transitioning are lacking.
Until now.
After describing Ontario’s gender medicine policies and where these interventions are provided, this article gives some insight into the extent of medical transitioning for minors in Canada’s largest province.
Policy
As with most other Canadian provinces, Ontario doesn’t regulate medical transitioning. Sherbourne Health, an organization that provides services “to people who may experience barriers to accessing health care” such as “2SLGBTQ people” runs Rainbow Health Ontario. Rainbow Health Ontario is the province’s leading promoter of medical gender transitioning. As part of their efforts, Rainbow Health Ontario publishes its own 136-page Guidelines for Gender-Affirming Primary Care with Trans and Non-Binary Patientsto help clinicians in their day-to-day practice. However, the document focuses on those who have completed puberty “and does not address considerations for trans and non-binary children or youth who have not completed puberty.”
The Guidelines promote an “informed consent model” for hormonal transitions rather than a traditional “gatekeeper model.” This informed consent model dispenses with any in-depth mental health assessment or referral process, though the Guidelines claim that this does not equal “hormones on demand.” Sherbourne Health claims that “new patients are usually seen for a number of visits prior to the initiation of hormone therapy,” though urgent cases are fast-tracked. A diagnosis of gender dysphoria or gender congruence is recommended prior to hormonal transition.
To be eligible for public funding under OHIP, a physician or nurse practitioner must fill out a Request for Prior Approval for Funding of Sex-Reassignment Surgery to be approved by the Ministry of Health. This form requires that a patient be assessed “by a provider trained in the assessment, diagnosis, and treatment of gender dysphoria in accordance with the World Professional Association for Transgender Health (WPATH) Standards of Care.” This assessment for “chest surgery” requires the diagnosis of persistent gender dysphoria for a mastectomy and a gender dysphoria diagnosis plus 12 months of continuous hormone therapy with no resulting breast enlargement (unless hormones are not recommended) for breast augmentation. For “genital surgery,” the assessment requires a diagnosis of persistent gender dysphoria, 12 continuous months of hormone therapy (unless hormones are not recommended), and 12 continuous months of living in their new gender role.
These are not legal requirements, however. They are funding requirements. It is perfectly legal to perform a sex-denying surgery on a minor who doesn’t have a diagnosis of gender dysphoria, who has never been on cross-sex hormones, or lived in their “new gender role.” Those requirements must only be met if the surgeon or patient wants the government to pay for their surgical transition.
Ontario covers the cost of puberty blockers, cross-sex hormones, and most “top” and “bottom” gender surgeries for minors if the proper forms are submitted. Some chest contouring and breast augmentation procedures are not publicly funded.
Providers
Puberty blockers and cross-sex hormones are relatively easy to access in Ontario. Many primary care providers (i.e. family doctors) now prescribe them to children and adolescents. One study with data collected in 2009-10 found that 67% of trans-identifying people in Ontario who were hormonally transitioning were prescribed these hormones by their family doctor. Rainbow Health Ontario believes that percentage “is almost certainly greater now.”
But if a family doesn’t have a family doctor who is willing to prescribe hormones, many community health clinics offer them. For example, Northern Ontario’s Gender Diversity Clinic, York’s Gender Affirming Health Clinic, Kingston’s Transgender Health Program, Durham’s Gender Care Team, Chatham-Kent’s Youth Gender Diversity Clinic, and Thrive Kids’ Clinic’s Gender-Affirming Pediatric Care program in Toronto all explicitly say on their websites that they prescribe puberty blockers and cross-sex hormones to children and adolescents.
There are also four hospital-based gender clinics in Ontario. SickKids Hospital Gender Clinic in Toronto, “one of the largest transgender youth clinics in Canada,” and CHEO’s Gender Diversity Clinic in Ottawa garner the most attention. But the London Children’s Hospital’s Gender Pathways Service and McMaster Children’s Hospital Adolescent Medicine Clinic provide hormonal transitioning to children as well.
Gender surgeries are primarily performed at the Women’s College Hospital in Toronto and the Ottawa Hospital. The Women’s College Hospital began offering gender surgeries in 2018, claiming to be the “first public hospital-based surgical program in Canada focused on providing safe and timely access to gender affirming surgical care.” It offers most “top” and “bottom” surgeries. The Ottawa Hospital’s gender-affirming surgery clinic opened in 2023, offering not only “top” and “bottom” surgeries but also facial feminization and masculinization surgeries. That hospital claims that “it is the only clinic in Ontario and the second in Canada to offer all three” types of procedures.
Specialty clinics such as Catalyst Surgical and GraceMed are dedicated to exclusively providing gender surgeries, with GraceMed alone claiming to have performed over 2,500 gender surgeries since 1988. Other plastic surgeons and clinics across the province also list “gender-affirming surgeries” among their wider cosmetic offerings.
Prevalence
It is challenging to find data on the number of minors who are medically transitioning in Ontario. The ideal dataset would reveal the full number of minors currently prescribed puberty blockers or cross-sex hormones for the purpose of a gender transition, plus the number of “gender-affirming” top and bottom surgeries performed on minors each year. But there are a couple of factors that make such data difficult to collect.
First, so many players are involved in gender medicine – children’s hospitals, specialized gender clinics, and family doctors. Not everyone involved in providing gender medicine is reporting all the needed data. And so, the little data available is often only a few puzzle pieces of the entire picture. Second, because all the medications or surgeries prescribed for a gender transition are also used to treat other conditions (e.g. precocious puberty, breast or prostate cancer, menopause, or naturally low hormone levels), it is difficult to isolate prescriptions for “gender-affirming care.” For example, it is relatively straightforward to find the number of prescriptions of testosterone through a public drug plan. But that data isn’t very helpful when the reason for prescribing testosterone isn’t listed in the data.
Because of all of this, the government doesn’t publish comprehensive data on medical transitioning anywhere. In most cases, that’s because the government doesn’t have the information. They simply let the system of medical transitioning carry on.
A couple of FOI requests to the government of Ontario confirm this. The government confirmed that they do not comprehensively track the number of minors receiving puberty blockers or cross-sex hormones at community health clinics from family doctors. However, the Ministry of Health began receiving data on the number of children and adolescents served at the four hospital-based gender programs. Due to a lack of reporting, the only total that we can report with certainty is that these hospital-based pediatric gender clinics saw 1,430 children in 2023-24. The Children’s Hospital of Eastern Ontario (CHEO) in Ottawa saw more than half of those patients. And in three of the four comparative years, the number of minors visiting these clinics increased from the previous year.
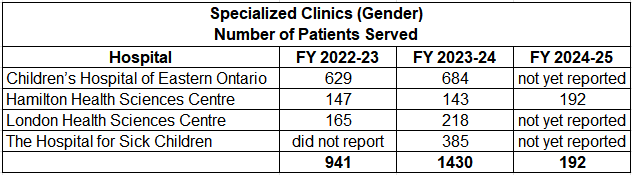
These numbers, however, are just the tip of the iceberg. They do not include the number of children and adolescents seen at community gender clinics or by family doctors. Remember that as far back as 2009-2010, two-thirds of hormonal transitions were prescribed by family doctors, and that figure is likely much higher today. If family doctors still see two-thirds of all children with gender dysphoria and community gender clinics see as many children as the hospital-based clinics, the number of children seeking medical help for gender dysphoria would be approximately 8500 a couple of years ago.
Furthermore, Ontario stated that it does “not track SRS [sex reassignment surgeries] performed in-province.” Ironically, they do track such surgeries performed out-of-province and even out-of-country.
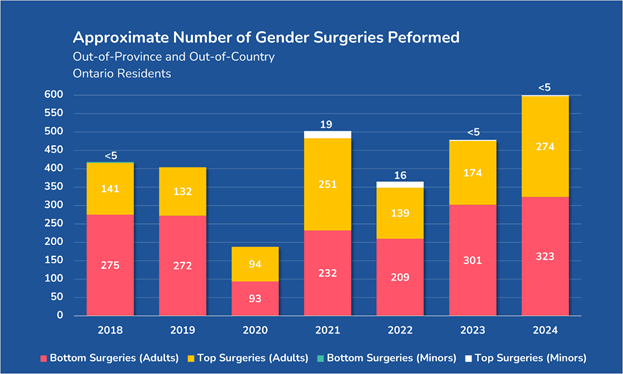
From 2018-2024, Ontario sent almost 3,000 individuals out of the province and even out of the country for gender surgeries. That averages out to about 420 per year. For the sake of context, Ontario sent more residents out of the province for gender surgeries than the province of Alberta performed last year. Now, Ontario doesn’t send patients out of the province for these surgeries because no institution provides them in Ontario. As mentioned above, hospitals and gender surgery clinics provide the full gamut of gender surgeries in the province. Patients were likely sent out of the province and out of the country because there was too much demand for these surgeries for these Ontario hospitals and clinics to handle. Sending patients outside Ontario allowed them to get surgery faster.
The government did not release the locations of where these surgeries occurred, but most out-of-province surgeries likely occurred at GrS Montreal, which is well known for handling gender surgeries for people around Canada.
Relatively few gender surgeries (roughly 40) were performed on minors out-of-province or out-of-country over the last few years. In 2018, fewer than five minors were sent out of the country for a phalloplasty. (Ontario lists numbers between one and four as <5, which makes data less precise but protects individuals’ privacy.) Nineteen minors received mastectomies out of province in 2021, sixteen more in 2022, and fewer than five in both 2023 and 2024.
Many gender ideologues claim that gender surgeries are not performed on minors in Ontario. But the above data demonstrates that minors from Ontario have been operated on out of province, paid for by OHIP. And while there is ironically no data on gender surgeries performed within Ontario (even though we have data on out-of-province surgeries for Ontarians), with no legal or clinical rules against it in Ontario, such surgeries have likely happened here too.
Conclusion
There are no legal restrictions on medical transitioning for minors in Ontario. The non-governmental organization Rainbow Health Ontario provides guidelines for clinicians, but its guidelines don’t address age restrictions. Puberty blockers, cross-sex hormones, and most “top” and “bottom” surgeries are eligible for public funding through OHIP, provided that a person is diagnosed with persistent gender dysphoria. In some cases, a twelve-month waiting period is required as well.
Unfortunately, only some of the data on children who are medically transitioning is available. Over 1,400 children visited hospital-based gender clinics in 2023-24. Many more visited community gender clinics or their family doctor. Approximately 40 minors received mastectomies out-of-province in the last few years, and up to four minors received bottom surgeries out-of-country in 2018. No data is available on the number of gender surgeries performed in the province.